What is PH
Definition and classification
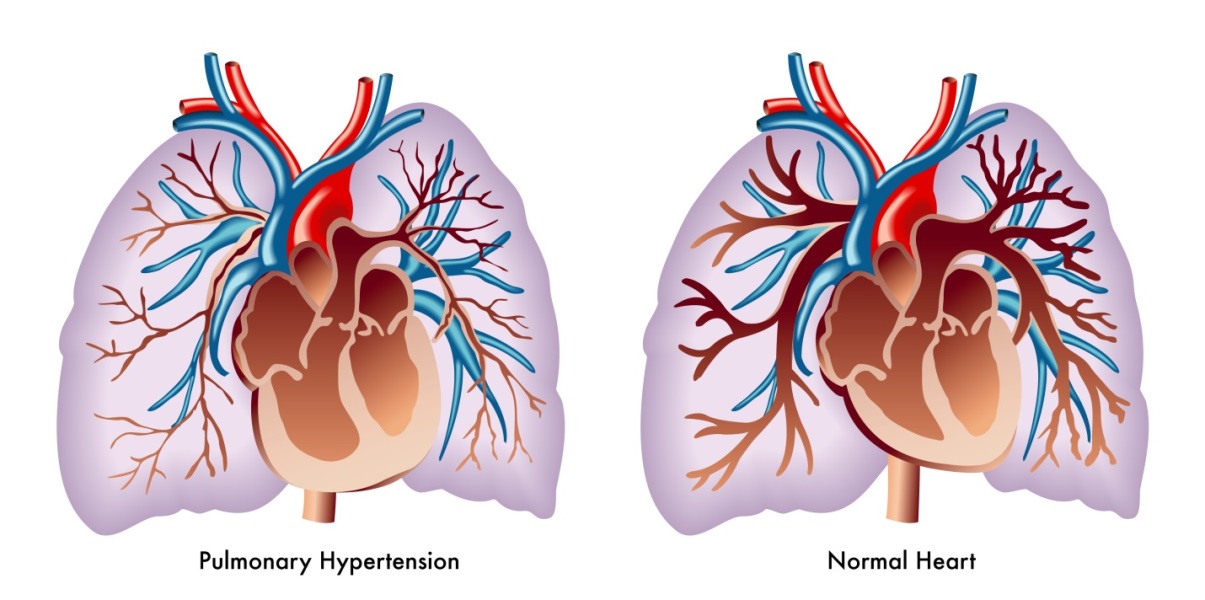
Pulmonary hypertension (PH) is a progressive disease, which is often associated with increased mortality. It is defined as an elevated mean pulmonary arterial pressure (mPAP) ≥25 mmHg at rest. Initial symptoms are typically exercise-induced and include shortness of breath, fatigue, weakness, angina and syncope.
There are five classifications of PH, which categorize the multiple clinical conditions based on similar characteristics of clinical presentation, pathological findings, hemodynamics and treatment strategy. In summary, these classifications are:
- Group 1: pulmonary arterial hypertension (PAH)
- Group 2: pulmonary hypertension due to left heart disease (PH-LHD)
- Group 3: pulmonary hypertension due to chronic lung disease and/or hypoxia
- Group 4: chronic thromboembolic pulmonary hypertension (CTEPH) and other pulmonary artery obstructions
- Group 5: pulmonary hypertension with unclear and/or multifactorial mechanisms
Disease mechanism
The mechanisms governing disease initiation differ between the PH subcategories. However, the drivers of disease progression that are responsible to varying degrees in each group include:
- Vasoconstriction
- Dysregulated cell growth
- Inflammation
- Thrombosis
PH is a complex, multifactorial disorder. Although there has been considerable progress made in understanding the molecular mechanisms involved, further research is required to better understand its pathophysiology, especially in the non-PAH subgroups. For further reading, please see Wilkins et al. 2012.
Treatment
In recent decades, there has been a significant advancement in understanding PH pathogenesis, which has led to the development of novel therapeutic targets. A comprehensive guide to PH therapeutic management strategies in relation to disease classification can be found in the published ESC/ERS guidelines for PH, as well as in the Proceedings of the 6th World Symposium on Pulmonary Hypertension (WSPH) 2018 in Nice. Below we present a summary of the current treatment strategies in PH.
Group 1: pulmonary arterial hypertension (PAH)
There are three well-characterized signaling pathways in PAH - the endothelin, the nitric oxide and the prostacyclin pathways, as shown in the figure below. Therapies are available to target each of them, with possible synergistic treatment benefits from using more than one in combination. The 2018 Nice Proceedings include an evidence-based treatment algorithm, which recommends combination therapy based on the individual patient’s risk assessment and their response to treatment. Recent data suggest that this approach can provide more substantial disease control and is thus being routinely used in many centers.
Group 2: pulmonary hypertension due to left heart disease (PH-LHD)
PH is a frequently occurring symptom of LHD (PH-LHD). The primary goal of PH-LHD therapy is to improve the underlying condition prior to considering specific measures to treat PH.
Group 3: pulmonary hypertension due to chronic lung disease and/or hypoxia
Currently there is no specific therapy for PH associated with lung diseases. Long-term oxygen (O2 ) administration has been shown to partially reduce the progression of PH in chronic obstructive pulmonary disease (COPD), however pulmonary artery pressure (PAP) values rarely return to normal and the structural abnormalities of pulmonary vessels remain. The effect of long-term O2 therapy on PH progression in interstitial lung diseases is unclear.
Group 4: chronic thromboembolic pulmonary hypertension (CTEPH) and other pulmonary artery obstructions
CTEPH is caused by chronic obstruction of major pulmonary arteries as a consequence of major vessel thromboembolism. An algorithm for the treatment of CTEPH is provided in the 2018 Nice Proceedings.